
Reversibility of Puberty Blockers and Citation Laundering
Reversibility of Puberty Blockers and Citation Laundering
Fact checking the Canadian Paediatric Society Position Statement on transgender and gender diverse youth

The Canadian Paediatric Society Position Statement An affirming approach to caring for transgender and gender-diverse youth is often cited in support of the position that puberty blockers are reversible. In fact, the Position Statement is a blatant example of citation laundering. This is a practice of citing weak or irrelevant sources to support a statement in an article. This article is then cited by another article and the process continues until there are enough citations to create the illusion of a strong scientific consensus.
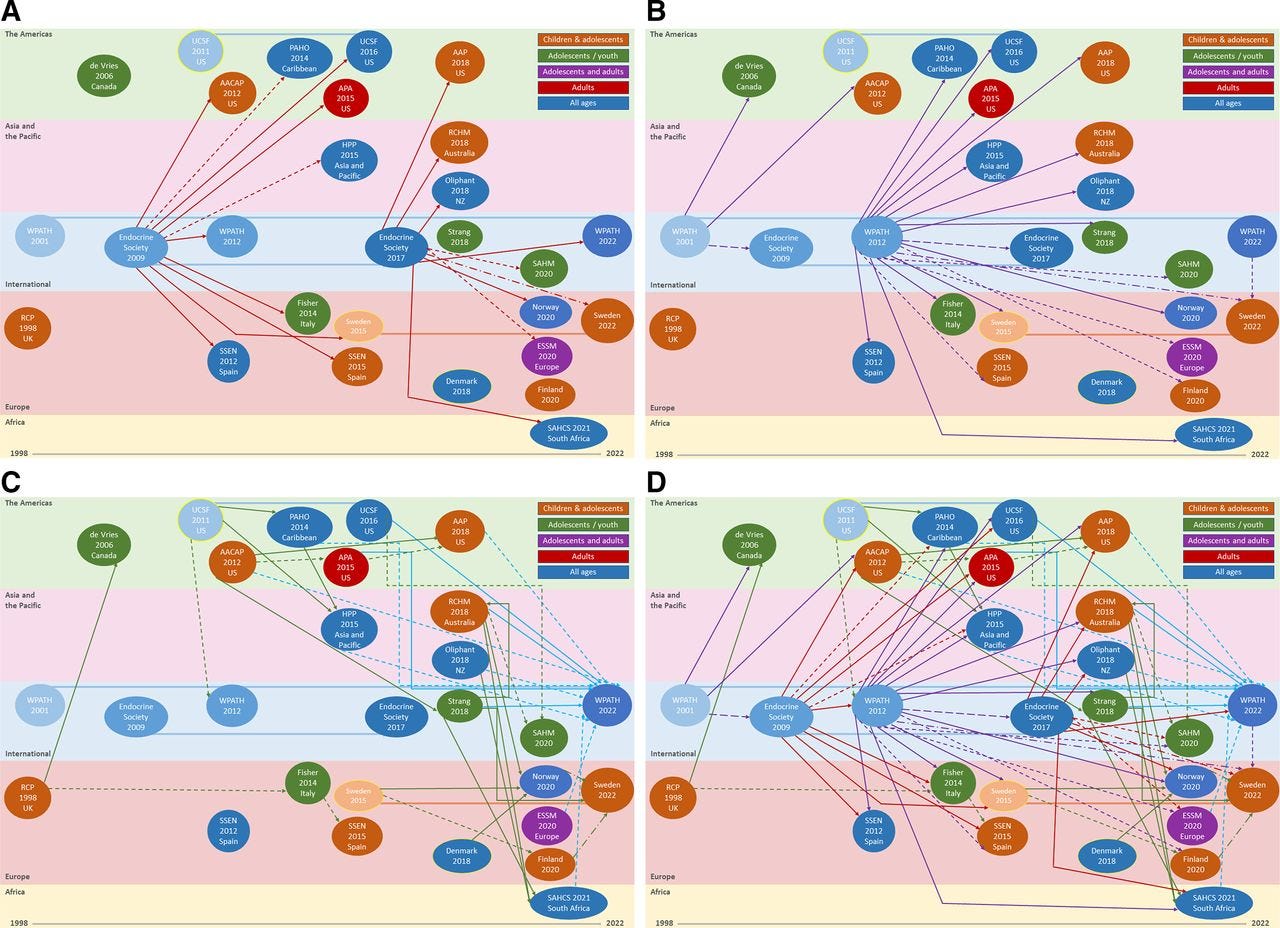
The World Professional Association for Transgender Health (WPATH) SOC 8 and the Endocrine Society Guidelines provide an example of citation laundering. The systematic reviews conducted in support of the Cass Review found that both WPATH and the Endocrine Society frequently relied on one another or on national guidelines which, in turn, had relied on early versions of the WPATH standards of care. The Canadian Paediatric Society Position Statement continues the cycle. It is not based on independent evidence review but relies heavily on WPATH, the Endocrine Society and the equally dubious American Academy of Pediatrics Policy.
The Position Paper also engages in citation laundering on more specific issues such as the reversibility of puberty blockers (which is refers to as hormonal suppression.)
Puberty blockers are drugs called gonadotropin releasing hormone agonists (GnRHA) which act to suppress the release of the hormones (testosterone or estrogen) which trigger the physical changes of puberty. Lupron is the most common drug used in North America.
Puberty blockers were first approved by the FDA for the treatment of precocious puberty in 1993. When used for this condition, the drugs are stopped when the child reaches the normal age for puberty (11 for girls and 12 for boys). Puberty will then proceed normally.
For the last 10 years puberty blockers have been used, off label, to treat children with gender dysphoria. It is claimed that by stopping the changes of puberty the drugs relieve a child’s anxiety about their body and give them more time to think about their gender identity. Puberty blockers for gender dysphoria are normally started when a child begins to show signs of puberty, which is normally around the age that they would be stopped when used for precocious puberty.
Gender clinics claim that puberty blockers for gender dysphoria are reversible based on the experience with precocious puberty but the two conditions cannot be compared. In precocious puberty, puberty blockers are used to correct an abnormally timed flow of hormones while in gender medicine they are used to disrupt a normally timed process.
There is no actual research which has found that children can have their puberty blocked during the normal window for puberty and then resume normal puberty without any permanent effects from the blockage. All studies of puberty blockers have found that more than 95% of children given puberty blockers for gender dysphoria proceed to cross sex hormones and never go through normal puberty.
While there are no actual studies which have found that the effects of puberty blockers during the normal window for puberty are reversible, there is evidence of possible serious irreversible effects including reduced bone density, loss of fertility and sexual functions and interference with brain development.
NHS England changed its guidance on puberty blockers to drop the claim they are reversible in 2020. In 2024 it changed its clinical policy to stop new precscriptions except in the context of a research study.
However, the Position Paper ignores these concerns and states:
Hormonal suppression is reversible, and endogenous sex-steroid production and/or effects will resume if hormone blockers are discontinued (62,64,85-89).
This statement skirts around the key controversy. It is true that that hormone production will resume once puberty blockers are stopped but that does not mean there has been no permanent effect. Puberty is a developmental milestone where there are many physical, psychological and social changes which are affected by sex hormones. If these changes take place without the normal flow of hormones there may be permanent effects wiich cannot be reversed later.
The list of seven references appears to give the statement weight, but if you examine each reference, you will see that not a single one refers to a clinical trial or even a case report which examines the effect of giving a child puberty blockers during the normal window for puberty and then discontinuing them without proceeding to cross sex hormones.
WPATH SOC8
Reference 62 is to the WPATH SOC8. It refers to “fully reversible puberty delaying blockers” at page S43 without any supporting references. Later on, it hedges a bit by warning that
Gender-diverse youth should fully understand the reversible, partially reversible, and irreversible aspects of a treatment, as well as the limits of what is known about certain treatments (e.g., the impact of pubertal suppression on brain development (Chen and Loshak,2020)) [p. S61]
However, it then goes on to make a strong recommendation for pubertal suppression with the following statement:
In general, the goal of GnRHa administration in TGD adolescents is to prevent further development of the endogenous secondary sex characteristics corresponding to the sex designated at birth. Since this treatment is fully reversible, it is regarded as an extended time for adolescents to explore their gender identity by means of an early social transition (Ashley, 2019e). Treatment with GnRHas also has therapeutic benefit since it often results in a vast reduction in the level of distress stemming from physical changes that occur when endogenous puberty begins (Rosenthal, 2014; Turban, King et al., 2020). [p. S112]
None of the four references in this paragraph contain any support for the claim of reversibility. Ashley 2019e is an opinion piece by Florence Ashley which contains no primary research. Rosenthal 2014 is a case report on two adolescents treated with puberty blockers. Neither patient had discontinued treatment at the time the article was completed. Turban, King et al. 2020 is an article on pubertal suppression and suicidal ideation based on data-mining a 2015 survey of transgender adults.
Note that the claim that puberty blockers result in a “vast reduction” of distress is questionable. The systematic review commissioned by the Cass Review, as well as all prior reviews, have found that the evidence of any benefits from puberty blockers is low certainty.
The Endocrine Society
Reference 64 is to the Endocrine Society guideline, which does attempt to cite some research in support of its claims. However, this research is not directly relevant as it does not deal with adolescents receiving puberty suppression for gender dysphoria.
For “those designated male at birth” the guideline claims that “prolonged pubertal suppression using GnRH analogs is reversible and clinicians should inform these individuals that sperm production can be initiated following prolonged gonadotropin suppression.” In support of this claim it cites one article on the effects of puberty blockers on males with central precocious puberty, and two articles (Buchter et al., 1998; Liu et al., 1999) on the treatment of adult men with gonadotropin deficiency. None of these studies consider the effects of blocking puberty in a physically healthyboy during the normal window for puberty.
For girls, the guideline makes the more cautious claim that “no studies have reported long-term, adverse effects of pubertal suppression on ovarian function after treatment cessation.” It cities two studies (Pasquino, 2008; Magiakou, 2010) on girls with precocious puberty.
Other References
The remaining references are to individual articles which have nothing to say about reversibility. Reference 85 (Vries et al., 2011) is to the initial Amsterdam clinic study on puberty blockers from 2011. All of the patients in this study either continued to cross-sex hormones and surgery or were lost to follow up. (Including one patient who died as a result of post-operative infection after a vaginoplasty.)
Reference 86 (Delemarre-van de Waal & Cohen-Kettenis, 2006) is to a 2006 article which describes the Dutch protocol and some preliminary results from the Amsterdam study. The article refers to puberty blockers as reversible but does not cite any supporting research. None of the patients referred to in the article had discontinued puberty suppression.
Reference 87 (Costa et al., 2016) is a review article which does not contain any new research. As support for its claim that puberty blockers are reversible it cites the Endocrine Society guideline and an article on the Amsterdam study which is Reference 89 in the CPS position statement.
Reference 88 (Cohen-Kettenis et al., 2011) is a preliminary report from 2011 by the researchers in the Amsterdam study which was published just prior to the article in Reference 85. It does not contain any additional evidence.
Reference 89 (Kreukels & Cohen-Kettenis, 2011) is another review article based on the Amsterdam study. This article is cautious in its claims. It says, “If treatment with GnRHa is stopped, puberty in line with the natal sex will continue to develop. In this sense, the treatment is reversible.” It does not cite any supporting research for this statement. This means that five of the seven references in the paragraph are based on the same clinical study which did not actually examine reversibility of puberty blockers.
And so, a statement with no supporting evidence receives the endorsement of a major medical organization. The Position Ptatement has not yet been cited in any peer reviewed articles but it is being referenced by the media and government agencies and relied on by practising doctors.
Excellent work. Its is amazing to see how captured these professional scientific societies are. 'Gender Affirming Care' is a just a re-run of the lobotomy story.
Good job!
I wonder if the observation that 95-98% of children started on puberty blockers will go on to cross-sex hormones without ever being given a chance to experience normal puberty could be chased down. What happened to the 3-5% of children who stopped PBs and *didn't* start hormones? Did their puberty resume, albeit late and stunted with bone loss and decreased IQ?
Or is this 95-98% figure just another oft-repeated statistic that is just someone's gut sense of what happens? There are no desistors to study because no one bothers to follow the kids who stop PBs and get lost to follow-up. A lot of that in this racket.