

Is Gender Exploratory Therapy Conversion Therapy?
A closer look at the Canadian law.

It is over a year since the amendments to the Criminal Code of Canada to ban conversion therapy passed with all party consent and much celebration. Since then there have been no actual charges under the law but this does not mean that it has been ineffective. The Department of Justice has been given a series of grants to organizations across Canada to produce educational materials on the law. These materials are now starting to appear and they make it clear that the fear that law would be used to enforce compliance with the gender affirmative model of care are well founded.
Concern about the effect of the law on the treatment of gender dysphoria will largely brush aside in the debate on the original Bill C-6. Although many of the 290 briefs submitted to the Justice Committee on the bill dealt with the issue of gender identity, it was barely touched on in committee hearings and the bill was approved without changes. When the Attorney General, David Lametti, appeared before the Justice Committee on Bill C-6, he gave the following assurances:
This means that the practices, services or treatments designed to achieve other objectives, such as abstinence from all sexual activity, combatting sexual dependency or criminal sexual behaviour—such as child sexual assault—are not clearly covered by the definition. Legitimate medical or therapeutic practices cannot enter into the definition either, such as interventions designed to support a person's gender transition, careful observation of young people whose gender identity does not match the sex assigned to them at birth, or detransition for those who choose.
Bill C-6 died on the order paper when an election was called and was reintroduced as Bill C-4. Although this bill had some significant changes from the previous one, the opposition allowed it to be passed without study or debate.
The materials now being published with Department of Justice funding contradict these assurances and call for a very broad interpretation of the law which would seriously restrict any approach to gender dysphoria other than the affirmative model of care.
Egale Canada (the Canadian equivalent of Stonewall or the HRC) has published a series of information sheets on conversion therapy. The first fact sheet paraphrases the law accurately but then adds, "the lack of treatment or service from a health care provider to provide gender affirming health care such as hormone replacement therapy (HRT), is also a form of conversion practice." A second fact sheet is even more explicit. It states that Cognitive Behavioural Therapy and Dialectical Behavioural Therapy and withholding "necessary medical care such as hormone blockers" may also be conversion therapy. A third sheet says that conversion therapy may be "disguised" in a variety of ways including:
· Reintegrative therapy
· Desistance therapy
· Sexuality counselling
· Healing sexual brokenness
· Gender exploratory therapy
· Encouraging relational and sexual wholeness
The documents appear to be based on the writings of Florence Ashley, a Canadian law instructor, who has proposed an extensive definition of conversion practices that would effectively prohibit anything except rigid adherence to the affirmative or “informed consent” models of care.
What is Gender Exploratory Therapy?
One type of therapy being targeted by the Egale materials is gender exploratory therapy. This is simply psychodynamic psychotherapy applied to clients with gender related distress as their primary concern. Therapists interested in this approach have formed the Gender Exploratory Therapy Association which recently publishes A Clinical Guide for Therapists Working With Gender Questioning Youth, which outlines the principles of gender exploratory therapy.
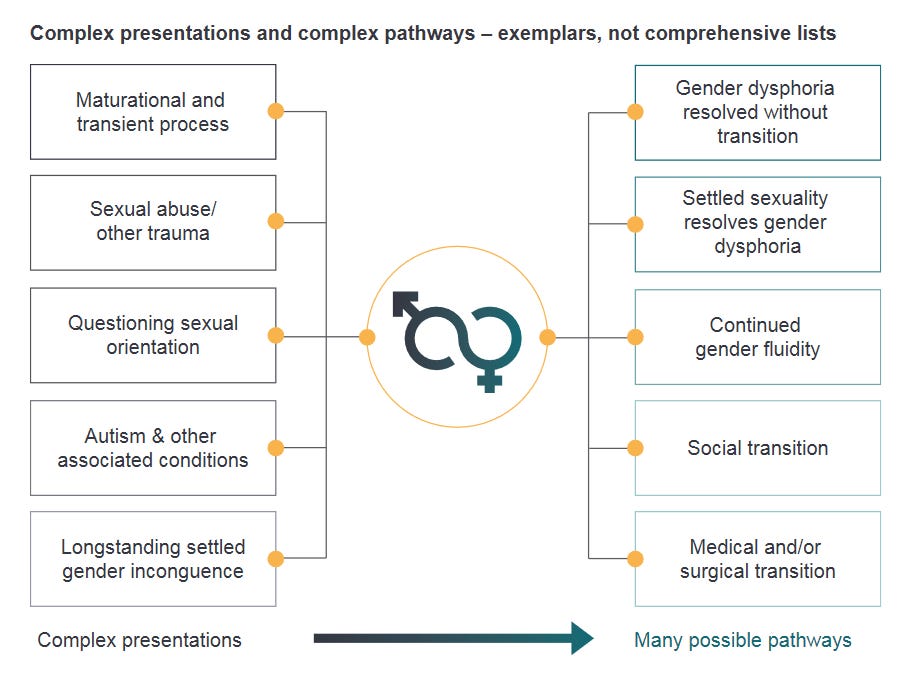
Gender exploratory therapy works with clients to resolve their gender related distress in a way that is both individualized and holistic. It looks at gender dysphoria through a developmental or biopsychosocial model. Gender dysphoria may have multiple causes and multiple possible outcomes. This approach is illustrated in a diagram from the interim report of the Cass Review.
Gender exploratory therapy is neutral as to outcome. The only goal is to relieve a client’s distress by reconciling mind and body. This can be done either by aligning the body with the mind or the mind with the body. Either approach is acceptable. The role of the therapist is to assist clients in making informed choices with a full understanding of all of the possible sources of their distress and all possible outcomes.
Gender exploratory therapists deny that what they do is conversion therapy. However, it may be more accurate to say that they deny that the concept of conversion therapy is relevant to gender identity. The term conversion therapy was originally applied to efforts to change sexual orientation. It has now been established that these efforts were ineffective and harmful. Sexual orientation is an innate characteristic which, once established, cannot and does not change.
The assumption that underlies the inclusion of gender identity in conversion therapy legislation is that it is also an innate and unchangeable characteristic. Gender exploratory therapy rejects this assumption. There is evidence that gender identity can and does change. Gender dysphoria can be the result of comorbid mental health conditions and may resolve if these conditions are treated. In other cases, it may be a part of a developmental process that will resolve into same sex attraction.
Gender exploratory therapists do not have the goal of avoiding medical transition. However, they do regard medical transition as something which not universally helpful and which may in fact do more harm than good. They therefore encourage an extensive assessment process to ensure that the client is able to give genuinely informed consent to the treatment.
What Would Happen in an Actual Case?
If a Canadian gender exploratory therapist were actually charged with practising conversion therapy, it would certainly be a difficult case involving a client with multiple mental health comorbidities where the therapist was visibly reluctant to encourage medical transition. The client would likely desist from transgender identification for a time during therapy and then re-identify and turn on the therapist after a mental health crisis.
The prosecution would have to prove that the therapist provided a service designed “to change a person’s identity to cisgender.” The therapist could respond that exploratory psychotherapy is not designed to attempt to identify and resolve the causes of a client’s distress. A client’s sense of identity may in fact change during therapy sessions, but this is the result of the client’s own self-reflection and not something the therapist seeks as an outcome.
The court will have to consider what gender identity and cis-gender mean. The Department of Justice has proposed these definitions:
Cisgender: People whose gender identity matches the sex that they were assigned at birth.
Gender: A person’s status in society as a man, woman, or as gender-diverse. A person’s gender may be influenced by several factors, including biological features, cultural and behavioural norms, and self-identity.
Gender identity: A person’s internal and deeply felt sense of being a man or woman, both or neither. A person’s gender identity may or may not align with the gender typically associated with their sex.
These definitions (which have no legal authority) are actually quite favourable to the defence. An identity which is internal and deeply felt is not necessarily the identity which the client presents to the world. Therapists can argue that their training and experience have taught them that the identity a client initially presents is often superficial or it may be influenced by unconscious factors the client does not fully understand. It is not possible to determine whether a client’s identity is internal and deeply felt without the benefit of exploratory psychotherapy.
The specific reference to a cis-gender identity also gives the therapist a great deal of wiggle room. Gender identities are not limited to transgender and cis-gender. A therapist could deliberately steer a client away from a transgender identity toward identifying as non-binary, gender-fluid, agender or any of dozens of possibilities with impunity.
Finally, the prosecution would have to prove that the therapy did not fall into the exclusion for “a practice, treatment or service that relates to the exploration or development of an integrated personal identity.” This exclusion is qualified by the proviso that the treatment is “not based on an assumption that a particular sexual orientation, gender identity or gender expression is to be preferred over another.”
The qualifier could be a problem in some cases. While the gender exploratory therapy is neutral as to outcomes, there may be times it may not always be possible to maintain strict neutrality throughout the therapy sessions. In these cases, the therapist will have to make the court understand that there is a distinction between regarding a particular gender identity as inferior or harmful and questioning whether a particular identity truly represents a particular client’s stable and deeply felt sense of self.
The Egale materials suggest that simple refusal to provide gender affirming care may amount to conversion therapy. This position would be even more difficult to establish in court. The law prohibits a treatment, practice or service, designed to cause change. This requires that the therapist some active steps. The claim that this language could also apply to refusal to provide a treatment or service would extend the words of the law well beyond their natural meaning.
On general legal principles, it would be very hard to bring a successful charge of conversion therapy for the practice of gender exploratory therapy. The presumption of innocence is strongly established in both common law and the Charter of Rights and Freedoms. In order to convict of an offence, it is necessary to prove both a criminal act and criminal intent beyond a reasonable doubt. There is considerable ambiguity in the wording of the law and this ambiguity should be resolved in favour of the accused.
However, there is a disturbing tendency to toss aside time-honoured principles where the transgender activist community is involved. If enough voices keep repeating that gender exploratory therapy is conversion therapy, there is a danger that judges and juries will believe them. This danger is particularly strong when some of these voices are major professional organizations.
Furthermore, in criminal charges against a professional, the process can be the punishment. The financial and personal cost of defending a criminal charge is extremely high and few therapists are prepared to run this risk. The practical result is that the effective scope of the conversion therapy law is going to be determined not by Parliament and the courts, but by propaganda from privately run but government supported groups like Egale Canada.
What Next?
Unfortunately, Canada’s conversion therapy law is going to be around for the foreseeable future. Even if the Conservative Party forms government after the next election, their leadership has not shown any interest in re-opening the issue. There is a possibility of challenging the law under the Charter of Rights and Freedoms, but success is not certain and therapists are understandably reluctant to become the accused in a test case.
The key to push-back will be through professional bodies at the provincial level. One of the peculiarities of the Canadian constitution is that while the making of criminal law is a federal power, proceedings in criminal matters are a provincial responsibility. This means that the decision to bring charges rests with the provincial Attorneys General. They would be unlikely to bring criminal charges for practices that the provincial professional associations believe to be ethical and appropriate care.
Given the positions that most professional bodies have taken on conversion therapy, this is small comfort. However, this is where change is most likely to begin. Positions that were adopted hastily, without much consideration, can be abandoned just as quickly. The prospect that they will be abandoned is increasing as international awareness grows of the weakness of the evidence base for affirming care and the harm suffered by detransitioners.
Yes, it is
https://journals.sagepub.com/doi/full/10.1177/17456916221102325?rfr_dat=cr_pub++0pubmed&url_ver=Z39.88-2003&rfr_id=ori%3Arid%3Acrossref.org&fbclid=IwAR1MWmFzQ0-BqpumU27Tc_A_IR2vKXPnpiFiz1GNJBo6jctxpY43XDgr7YY
Thanks, this is good information,.